
When it comes to COVID news, the last two weeks have been dizzying. The surge caused by the Delta variant has dominated local and national headlines, leading to new policy guidance at the state and federal levels and surfacing widespread anxiety and legitimate questions about what it all means. Do the vaccines still work? If I’m not vaccinated, should I get vaccinated now? Should I be wearing a mask indoors? Will I need a booster?
To help sort through this latest iteration of our COVID reality, I sat down for a conversation with David J. Roach, MD. Dr. Roach is an Infectious Disease Fellow at Harvard and Massachusetts General Hospital. He’s also my kid brother. Before moving to Boston, he spent the prior year treating hundreds of COVID patients at the University of Washington at Harborview Medical Center in the ICU. Before that, he was born and raised in Pasco. His answers here are his own opinions, and he is not speaking as a representative of Harvard or Massachusetts General.
John: The May CDC announcement relaxing the nationwide mask recommendation led to many people (myself included) easing into an actual, real summer routine that resembled what we’re used to. Widespread availability of vaccination in the US and drastically falling case, death, and hospitalization counts helped people to breathe easier, and even allowed the more obsessive COVID-trackers among us to ease up on the refresh button.
The Delta surge has snatched away that respite in breathtaking fashion, around the country but especially right here in the Tri-Cities. Here, we (once again) find ourselves atop the national rankings of regions with massive viral spread, and at the bottom of the vaccination rankings for our state. Our hospitals and ICUs are (once again) full to overflowing, and local patients needing an ICU bed are being shipped several states away for care. Old conflicts over masks and other public health interventions are heating back up, even as the disinformation war that has dominated our discourse for the past year and a half is further inflamed by the presence of vaccines in the mix.
So, on the subject of vaccines. The recent CDC report detailing the higher-than-expected prevalence of ‘breakthrough’ cases in vaccinated individuals has a lot of people worried. In your view, is this unexpected? Here at Kadlec in Richland, 99.5% of ICU patients are unvaccinated, but there is a narrative that the recent breakthrough cases mean the vaccines aren’t as good as we thought. Do the vaccines still ‘work’ against Delta?
Dr. Roach: YES! They absolutely still work. As you point out, the vast, vast majority of hospitalized patients are unvaccinated. Remember, when the vaccines were developed, the goal was to prevent moderate and severe illness, which they do incredibly well and which they continue to do. A secondary goal, and hope, was that they would help prevent transmission. They seem to do that well with the original strain and other variants, which was a BIG BONUS, above and beyond the original goal.
The Delta variant is different, in that data is showing that vaccinated individuals can still spread it. I think, though, that the widespread use of the term ‘breakthrough’ to describe vaccinated people being infected is a bit of a misnomer, because these infections rarely result in clinically-significant infections. These vaccines do prevent moderate and severe infections against all the known variants, including Delta, although we need further data in the coming weeks to confirm that this is the case.
John: With reinstatement of mask policies, there is a situation of ‘strange bedfellows’, with some resentment and frustration amongst both the historically anti-masking folks AND vaccinated folks who are now frustrated about having to mask again after having ‘done everything right’ over the last year. Do you think that we should be asking vaccinated folks to mask up in indoor settings, in light of what we’re seeing? Why do you think we’ve struggled so much to help people see that masking is not just about individual risk, but community risk?
Dr. Roach: Wearing a mask indoors in areas of high community spread like the Tri-Cities definitely makes sense from a public health standpoint. The challenge comes when you get into other possible restrictions, like social distancing requirements or closing down facilities. The risks and benefits of those types of interventions have changed with the availability of vaccines, so it’s a more difficult conversation. I think this is a very regionally-specific conversation. If the data changes and we start seeing a much higher rate of vaccinated individuals being hospitalized, that would change the conversation again.
John: This Delta surge is happening really fast — faster than policy can keep up, especially in areas of high spread like the Tri-Cities. It seems like rather than relying solely on government guidance, people should really be assessing their own and their family’s risk levels and tailoring their activities accordingly. What guidance would you give individuals and families in areas of rapid spread, but where everything is still ‘open’?
Dr. Roach: First, and most importantly, if you aren’t vaccinated, get vaccinated! Second, maybe consider that taking a pause for a few weeks on your normal indoor summer activities would be a good idea. Reinstate the same habits that you had in place last summer around social interactions and gatherings. And if you’re around someone who is at-risk, immunocompromised, or elderly with underlying conditions, remember that there is a non-zero chance you could spread COVID to them and adjust your behavior accordingly. I’ve seen that play out with dozens of my patients.
John: The rapid rise and the Delta surge in both India and the UK seem to suggest that this surge in the US may burn itself out more quickly than the sustained surge in the US last winter. Do you think that’s likely?
Dr. Roach: Well, I don’t really know, and I don’t think anyone does. COVID is weird, and we don’t understand everything about how it’s working. The US is very different from India and the UK. It’s very regional and has a very heterogeneous risk pool. India was highly unvaccinated, and the UK was actually quite highly vaccinated. Also, we don’t really know yet what’s going to happen with people who’ve had the original COVID variant and may be re-infected with Delta. So there are just too many unknowns for me to make a prediction.
John: What are you hearing about the likelihood of vaccine ‘booster’ shots becoming a recommendation?
Dr. Roach: I think it’s inevitable that this will happen, but it’s still unknown what kind of public health framework will guide this, and what metrics will be used to make the determination of when a booster is recommended.
John: What would you say to someone who is still vaccine-hesitant based on the fact that the vaccines are still not fully authorized by the FDA?
Dr. Roach: I think the number one thing to consider for those who are vaccine-hesitant, for whatever reason, is that any of the very rare complications one might be concerned about from the vaccine can also be caused by the virus itself, but they are much more severe (including death) if caused by the virus. I expect full FDA approval in a couple of months, but what we already know is that COVID can be very severe and have long-lasting symptoms, even in a significant percentage of those who survive it. So taking the vaccine actually gives you a much higher likelihood of avoiding complications or symptoms altogether.
John: In Washington, there is also concern about another variant, Gamma, which is associated with increased hospitalizations. I know different vaccines have different efficacy levels with different variants, but in general, what should the average person be thinking about in terms of the different variants?
Dr. Roach: I think this is one of those questions where you can really get lost in the weeds, and all the headlines around this topic don’t help. It’s really the epidemiologists' and the virologists’ job. But what should be understood is that all of the known variants of concern are responsive to the vaccines we have. They are your best bet to keep you and your loved ones safe. Also, it is not necessarily the case that further mutations will be more virulent. It could be the opposite, in fact. A more vaccine-evasive variant might actually be less virulent. As a society, we will have to remain vigilant with variant tracking and public health measures to continually assess these questions.
John: There is still a strong tendency to frame COVID in terms of binary outcomes — either death or survival — yet around 20% of patients are suffering from some types of long-term COVID symptoms, including impacts to brain function. What do you think about these risks, and do you think they should feature more prominently in the way we talk about COVID and the ways individuals assess their personal risks?
Dr. Roach: I absolutely think we should be more clear about these risks in the way we talk about COVID. I have to note, in the ICU, I’ve taken care of the sickest population of COVID patients, so I am biased in that regard. But many patients, whether they ended up in the ICU or not, have long-lasting problems no matter how sick they got. With their lungs, their muscles, and their brains. Even those who aren’t hospitalized have a much higher risk of a variety of diseases in the three months after COVID, and a significantly higher mortality rate. This could be due to having all of your blood vessels inflamed, and leads to a lot of downstream effects, even if you didn’t have COVID severely affecting your lungs.
So, many who have severe COVID pneumonia never get back to their prior function, and even if you don’t get pneumonia, you’re still often subjected to those downstream effects. This ‘lives versus dies’ metric that is so dominant doesn’t recognize the pain and suffering COVID causes to many who survive.
John: In the Tri-Cities, we’ve heard reports of severe burnout from nurses and other healthcare workers leading to staffing shortages that are impacting the ability to care for patients in this most recent surge. Have you witnessed this, and do you have any ideas how people can help alleviate it?
Dr. Roach: Yes! Everyone in the healthcare field involved with treating COVID patients is so frustrated, so tired, and so sick of it. It is very labor-intensive to treat COVID patients. In the first waves, we were seen as heroes, and it was heartwarming and sustaining. But as the misinformation has hardened, we are being put in the position of putting ourselves at risk to help people who seem to have invited this onto themselves. This is sad, and difficult, and frustrating. When you watch their family members watch them die, it wears on all of us. Especially when it could have been prevented. Many healthcare workers just have nothing left in the tank.
John: It seems like the former goal of ‘herd immunity’ is fading in light of the massive contingent of voluntarily unvaccinated individuals. What does that mean for our new goal? That COVID becomes endemic, and we manage it somewhat like the flu? What does that mean for the immunocompromised?
Dr. Roach: Look, even if we got to 70%–80% vaccinated in the US, which we’re a long ways from, we are nowhere close to that on the global level. COVID is here to stay and will be a major cause of mortality for years. We need to get vaccines widely deployed, so even if it is present and spreading, its disease profile is mitigated and transmitted like a mild flu. This should be our goal now.
John: How many doctors do you know who are unvaccinated?
Dr. Roach: ZERO.
John: Any other comments or thoughts for the people in your hometown?
Dr. Roach: A lot of people say, “It’s none of your business if I’m vaccinated.” But that’s not true. It is. Because if you get COVID, not only can you spread it unknowingly to others, but overflowing hospitals mean everyone is impacted. Every bed taken up by a COVID patient means a bed that’s not there for someone else. We talk about personal responsibility a lot in this country, and this is an opportunity for you to be responsible to yourself, and to your neighbors. I hope those who aren’t yet vaccinated see that and take advantage of it. Do it for yourself, and do it for others.
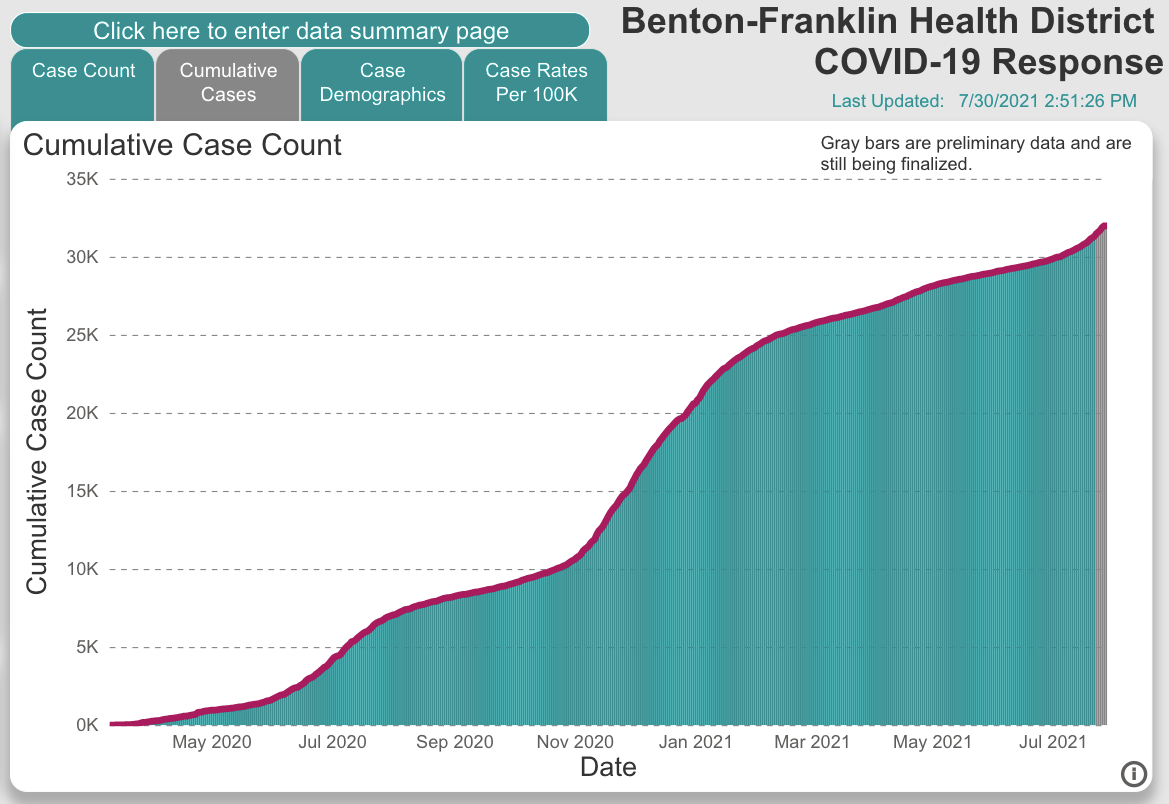
Graph data from covid19.bfhd.wa.gov